Subscribe if you want to be notified of new blog posts. You will receive an email confirming your subscription.
The Real Secret Sauce of Medicare’s Participation in Regional Collaboratives — Network Effects
Last week I asked whether Medicare’s Biggest Change in 40 Years is on the horizon. That post described and discussed implications of Medicare’s new direction for the medical home — the shelving of Medicare Medical Home Demonstration (MMHD) and the refocusing on the recently announced Multi-Payer Advanced Primary Care Initiative (MAPCI).
In that post I touched briefly on the potential for MAPCI to create effective networks at multiple levels — contracting networks, health IT networks, social and collaborative care networks. I’d like to expand a bit today…
So, why is Medicare’s participation in MAPCI and other regional collaboratives such a big deal? Here’s my hypothesis:
Medicare’s non-participation (to-date) in regional payer/provider collaboratives has been a rate limiting factor in the potential to achieve high levels of network effects that drive adoption.
A Non-Healthcare Example
As I’ve referenced in another series of blog posts, healthcare has much to learn from the developing practice and science around 1) the economics of networks and 2) platform/application business models.
Let’s consider a non-healthcare example: think about the value you might place on a credit card from Home Depot (that you can only use at Home Depot) vs. a Mastercard (that you can use almost anywhere).
-
The potential for network effects and broad adoption for the Home Depot card is minimal to moderate — it’s limited by the number of Home Depot locations, by the relatively small number of people who care to shop there, and because you can’t pay for your dinner with a Home Depot card.
-
The level of network effects and broad adoption for Mastercard is large — Mastercard’s deep penetration of vendor acceptance drives consumers to the card, and vice versa. Vendor acceptance and consumer acceptance are mutually reinforcing.
Medicare and Network Effects
Think about a regional health care delivery through the lenses of network economics. I’ll keep it simple.
Overall, Medicare pays for a total of 40–50% of all health care services provided by doctors and hospitals. This varies by specialty and region — but it’s in the ballpark. Thus, doctors and hospitals have to pay a lot of attention to Medicare because as a payer its such a large proportion of their revenues.
…and the the converse is true as well: doctors and hospitals don’t pay a lot of attention to payers that aren’t a large proportion of their revenues. This realization is the driver behind current experimentation with multi-payer initiatives occurring in many regional markets.
While well intentioned, existing multi-payer initiatives are severely hamstrung because the biggest dog in the payer neighborhood — Medicare — hasn’t been at the negotiating table.
Consider three scenarios of how payers might interact with physicians:
- One payer with 10% regional market share tries to dictate adoption of proprietary evidence based guidelines
- Multiple payers with 30% regional market share (but not including Medicare) collaboratively influence development and implementation of evidence based guidelines
- Multiple payers with 75% regional market share (including Medicare) collaborate in creating public-utility like infrastructure for care and care management
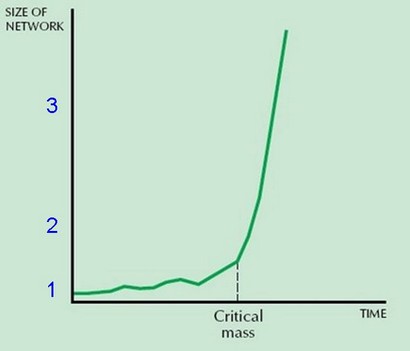
Which of these has ability to move a market, and why? The diagram below places each scenario on a map of potential network effects.
NETWORK EFFECTS
1) One payer with 10% regional market share tries to dictate adoption of proprietary evidence based guidelines (e.g., for diabetes care).
What happens? Nothing. The FedEx effect is at work, and here’s what we hear from doctors:
“My complaint is that this guideline is dumped at my doorstep. I’ve had no input into it. I have no systems in my practice to implement it. I participate in contracted provider networks for a dozen different plans. Each of them has given me clinical guidelines for multiple conditions; each of the guidelines is in a different format and contains differences in recommended treatment approaches. I don’t get paid for all the extra work that would be involved. There’s no way I can keep track of all this! Maybe it’s true that guidelines could improve patient care, but darn it—I resent that anyone tells me how to practice medicine. And if I took the time to know all this stuff, I’d have no time for treating real human beings.”
2) Multiple payers with 30% regional market share (but not including Medicare) collaboratively influence development and implementation of evidence based guidelines.
What happens? This scenario is occurring today in many multi-payer initiatives. The potential for successful collaboration is high; a poster child for success has been collaborative initiatives driven by the Institute for Clinical Systems Improvement (ICSI) in Minnesota. ICSI has brought together 56 medical groups, 6 large payers, and major delivery systems.
But the potential for expanded adoption and network effects is constrained — by definition Medicare isn’t sitting at the table and 50% of doctor and hospital revenues can’t be influenced by today’s multi-payer collaboratives. It’s like the Home Depot credit card example — how much attention do you pay to a credit card that has such limited uses?
3) Multiple payers with 75% market share (including Medicare) collaborate in creating public-utility like infrastructure for care and care management
What will happen? We don’t know…it’s never happened.
But this is the scenario MAPCI initiatives promise to create.
Common sense tells us that doctors and hospitals would have to pay a lot of attention to this collaborative. Network effects kick in because this type of collaborative could cover almost all the patients in a doctor’s practice.
The potential to develop networks at many levels — contracting networks, health IT networks, social and collaborative care networks — is greatly enhanced.
Is Medicare’s Participation in Regional Collaboratives a “Nice to Have” or a “Must Have”?
Again, we don’t know…but it’s an important question to ask.
The payment structure of Medicare to date has pretty much ignored the question.
Medicare’s participation in MAPCI demonstration projects promises to create truly effective “networks”…the potential is huge!
This work is licensed under a Creative Commons Attribution-Share Alike 3.0 Unported License. Feel free to republish this post with attribution.
Medicare's new medical home model–multipayer collaboratives drive network effects http://bit.ly/2Q74Ql #PCMH #healthreform #healthit
Good read RT @VinceKuraitis: Medicare's new medical home model–multipayer collaboratives drive network effects http://bit.ly/2Q74Ql #PCMH
RT @VinceKuraitis: Medicare's new medical home model–multipayer collaboratives drive network effects http://bit.ly/2Q74Ql #PCMH
The Real Secret Sauce of Medicare's Participation in Regional … http://bit.ly/4CwrmE
The Real Secret Sauce of Medicare’s Participation in Regional Collaboratives — Network Effects (@VinceKuraitis ): http://bit.ly/w7fnM
The Real Secret Sauce of Medicare’s Participation in Regional Collaboratives — Network Effects (@VinceKuraitis ): http://bit.ly/w7fnM
Hi Vince,
I would love to see your discussion of network effects continue. The first 3 articles in your the series were great.
It makes me think of account-driven healthcare plans, and wonder how that trend will be impacted by network effects. According to recent EBRI report, 4% of adult population has these; an additional 4% are eligible high deductible plan holders; and they are growing at about 1% of adult population per year.
These accounts all tie back to financial institution custodians, which have been grappling with network effects for a few more decades than the healthcare system. Sure, Mastercard is a success, and we get secure realtime financial data through a great many channels, but the drama continues in many respects.
Software vendors that run the core central information file control the nervous system of community financial institutions. Some are cloud-based, but API interconnectivity comes with a surcharge. Famous ones with names like Open Systems are anything but.
Ultimately the account data in account-based health plans is going to need to network with the broader healthcare system.