Subscribe if you want to be notified of new blog posts. You will receive an email confirming your subscription.
Is HITECH Working? #2: Key physicians will sit on the sidelines (at least for now).





(click on any of the above graphics to be linked to the orginal source)
by Vince Kuraitis JD, MBA and David C. Kibbe MD, MBA
In the previous post in this series on “Is HITECH Working?”, we straightforwardly noted that hospitals are playing in the HITECH game. The issue of whether physicians will play is MUCH thornier.
As the headlines above succinctly convey — we conclude that for now there is too much fear, uncertainty, and doubt (FUD) to expect significantly increased EHR technology adoption by most physicians from the HITECH incentives and penalties.
Here are topics we’ll cover today:
- Fear, Uncertainty, Doubt
- Little Risk by Waiting a Year or Two
- A More Granular View — Segmenting Physicians
- Is There Another Side to the Story?
- How Important is Physician Adoption to the Success of HITECH?
Fear, Uncertainty, Doubt
What’s the physician FUD all about? Here are some concerns about HITECH as they might be voiced by physicians:
My early adopter colleagues have horror stories about their EMR (electronic medical record) software systems.
The costs outweigh the benefits. HITECH financial incentives aren’t significant enough to bother with.
My workflow will be disrupted and productivity will decline, and this isn’t tolerable when payment from Medicare and Medicaid is shrinking.
The current generation of EMRs are not user-friendly, in fact, their downright difficult to use.
The adoption time lines for meaningful use are too aggressive.
The benefits of EHRs accrue primarily to insurance companies and government, not me.
I don’t trust the government. Look what a mess PQRI turned out to be.
The reporting burdens are a hassle.
I understand there are potential penalties in 2015, but the government would never clamp down on physician reimbursement – we’re too important.
I’m really confused about what “certified EHR technology ” really means. Who is certifying, and what’s this I hear about EHR modules?
Prices of EHRs will come down…let’s wait.
I’ve been hit by the recession. Patient visits are down and I don’t have the money to invest.
Will the EHR I buy be interoperable with the hospital next door? So far that hasn’t happened, despite a lot of promises by the industry.
Will the EHR be interoperable with ALL the hospitals in the community?
What? I don’t get any money up front to buy an EHR?
Will I buy the wrong EHR technology, and then be locked in?
What will ONCs final rules for meaningful use (MUY) look like?
What extra burdens will be added by Phase II & III MU objectives? These are complete unknowns.
Little Risk In Waiting A Year or Two
So…there are many reasons NOT to proceed. Is there a risk of waiting a year or two?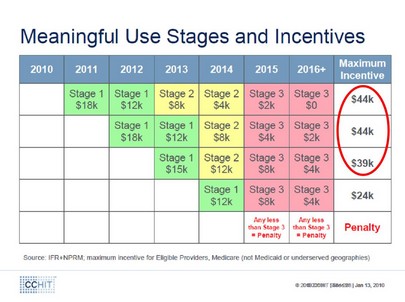
Source: Certification Commission for HIT (CCHIT); click on the diagram to see a larger version)
As shown by the above chart , there is NO overall penalty in waiting one year — a physician can still claim the entire $44K incentive payment, and there is minimal penalty in waiting two years (only a $5K loss from $44K to $39K).
A More Granular View — Segmenting Physicians
HITECH does not appeal to or impact all physicians equally. Let’s look at several prototype segments of physicians to see how they might be affected:
- Large Physician Groups
- Small/Medium Primary Care Practices
- Specialists
- Hospital-Based Ambulatory Care Physicians
1) Large Physician Groups. Characteristics of this group include:
- 26+ physicians in the group
- Mindset: sophisticated business practices; likely to have professional practice manager
- EMR adoption already is high (e.g., a recent SK&A survey found “usage of EHR software” to be 71% in groups of 26+ physicians)
- Only a small minority of physicians practice in large groups. (A recent CDC Report noted that only 11% of physicians practice in groups of 11 or more; see table 1.)
Large physician groups are the most likely to pursue HITECH funding incentives. However, since EMR adoption in this group is already high, the incremental number of new adopters is limited. HITECH could become a windfall for some large physician groups.
The incremental opportunity to improve care coordination in a large group with an EMR is low. Physicians in large groups mostly will be making referrals to other physicians within their own group — not to unaffiliated community physicians. A large physician group with their own EMR is already able to exchange data within their group.
2) Small/Medium Primary Care Practices. Characteristics of this group include:
- 10 or fewer physicians
- Mindset: individuals rather than strong sense of “organization”; will have staff for administrative functions, but unlikely to have a professional practice manager.
This segment of physicians is highly influential in overall community EHR adoption and should be a high priority target for HITECH:
- The vast majority of primary care is provided by small/medium practices
- Primary care physicians with EHR technology can be influential in encouraging specialists to whom they refer patients to adopt EHRs
- These physicians have the greatest opportunity to improve care coordination; the vast majority of referrals will go outside of the group. Interoperable EHR technology will needed to share data and workflow across physician practices.
However, small/medium physician practices are least likely to take advantage of HITECH incentives:
- The administrative burdens will be disproportionally large. These groups have little technical or administrative infrastructure.
- Concerns of productivity loss will be high.
- FUD factors will weigh heavily.
3) Specialist Physicians. Characteristics include
- Have significantly higher incomes that primary care physicians
- Have lower EMR adoption rates than primary care physicians (as documented by a recent CDC Report; see Technical Notes Table)
We question whether HITECH incentives are significant enough to motivate adoption of EHR technology; specialists make most of their money through tests and procedures, not by coordinating care. We find the perspectives of Evan Steele, CEO of SRSsoft, to be highly persuasive:
It has been abundantly clear to me that the government’s EHR program is not relevant for specialists and other high-volume physicians. It was evident from the outset that specialists were never the focus of the legislation, but recent program-funding announcements dispel—once and for all—any doubts about the government’s intentions in this regard. Furthermore, the type of EHRs that are designed to meet the government’s criteria are not responsive to the particular needs of specialist physicians. The comments I continue to receive, and those posted elsewhere, are adamant on that point.
4) Hospital-Based Ambulatory Care Physicians
- Approximately 13% of family practice physicians are in this category
- Proposed HHS rules exclude these physicians from receiving HITECH incentive payments (see Brian Ahier’s column in healthsystemcio.com for a discussion of this issue)
HHS has developed an excessively narrow definition of hospital-based eligible providers. Many who have commented on the Notice of Proposed Rule Making for Meaningful Use have noted that there is no reason to exclude hospital based-ambulatory care physicians from receiving HITECH incentives. We agree.
[UPDATE: On April 15, President Obama signed legislation allowing hospital-based ambulatory physicians to be eligible for HITECH incentives. Click here for details.]
Is There Another Side to the Story?
We do want to acknowledge the other POV on the issue of physician EHR technology adoption.
There are a fair number of experts who DO predict physician uptake of EHRs. We could be wrong, and we hope we are.
For example, a recent Accenture survey of physicians found that 58% of physicians who don’t use EMRs anticipate adopting in the next two years.
Here’s our comeback to this and similar surveys. Many physicians who answer these surveys are like car buyers on a first visit to a showroom lured by the promise of large factory rebates. They’ve yet to do their homework, look under the hood, and calculate the total cost of ownership.
The FUD hasn’t kicked in yet. Expressing an intention to purchase isn’t the same thing as actually purchasing.
How Important Is Physician Adoption to the Success of HITECH?
It’s absolutely critical.
- Physicians are the key to cost reduction and quality improvement
- Patient day-to-day continuity of care is coordinated by physicians using EHR technology; patient contact with hospitals is far less frequent
Recall The Penguin Problem in one of Vince’s previous blog posts. Economists describe it as: No one moves unless everyone moves, so no one moves. The point here is the importance of expectations in predicting the adoption of a network technology (i.e., EHRs). Many physicians and hospitals have been reluctant to be first movers because they have doubted others will be following.
The strong FUD being experienced by physicians is the opposite of the strong expectations of peer adoption needed to pass the tipping point in a market with strong network effects.
Let’s recap: FUD is very high. Physicians risk little by sitting on the sidelines — at least for a year or two. While small/medium primary care practices potentially have the greatest leverage in community EHR adoption, they are least likely to participate in HITECH as currently structured.
How big a deal is physician non-adoption? It’s a potential deal-breaker for the success of HITECH. We’ll discuss options in the final post of this series.
Survey: Healthcare Information Technology Adoption Among Small Physician PracticesNaviNet, March 2009
Letter to CMS re: Meaningful Use NPRM
signed by AMA and 95 other physician organizations; March 15, 2010
Letter to CMS re: Meaningful Use NPRM
American Academy of Family Physicians; February 26, 2010
The Cost of Fear
Musings of a Distractable Mind blog; January 27, 2010
It’s Not About Meaningful Use
John Moore, The Health Care Blog; March 12, 2010
2010 Physician Sentiment Index
AthenaHealth & Sermo, March 2010
This work is licensed under a Creative Commons Attribution-Share Alike 3.0 Unported License. Feel free to republish this post with attribution.
Is HITECH Working? #2 : Key physicians will sit on the sidelines (at least for now). http://bit.ly/a9sJiR #healthit #ehr
RT @VinceKuraitis: Is HITECH Working? #2 : Key physicians will sit on the sidelines (at least for now). http://bit.ly/a9sJiR #healthit #ehr
@VinceKuraitis Enjoyed your post “Is #HITECH Working? #2” & appreciate mention in Specialist Physicians section. http://tinyurl.com/yespmzb