Subscribe if you want to be notified of new blog posts. You will receive an email confirming your subscription.
Is HITECH Working? #3: ONC got it right on the 3 major policy interpretations: Meaningful Use, Certification, Standards
We concluded our last post in this series with a blunt prediction that “key physicians will sit on the sidelines” and that clinician non-adoption of EHR technology is a potential “deal-breaker for the success of HITECH”.
While this might sound like a criticism of the way HITECH has been implemented, it’s not intended that way — it’s a commentary on 1) the complexity and scope of change that will be required to make HITECH successful, and 2) the level of protective entrenchment existing American health care today.
Rather, we believe that the Office of the National Coordinator (ONC) for Health IT – Dr. David Blumenthal and his staff — have done a superb job in interpreting and defining key aspects of HITECH legislation. We’re big fans.
For those of you who have been following our writings over the past 18 months, think of this post as a summary and status report on the extensive incumbent (cat) vs. innovator (dog) dialogue:
-
A Recap — The Stagnant Electronic Medical Record (EMR) Market Before 2009
-
ONC Gets It Right In Three Major Interpretations and Definitions of HITECH
a) Meaningful Use (MU) Emphasizes “Meaningful”, Not “Use”
b) Vendors Get a Level Playing Field With Certification
c) Lightweight, Open Standards Promote EHR Interoperability and Modularity
1) A Recap — The Stagnant Electronic Medical Record (EMR) Market Before 2009
Remember what the EMR market looked like before 2009?
- Hospital and physician EMRs were monolithic. EMRs came with predefined functionality that was difficult and expensive to modify and did not allow for addition of new, innovative modular applications.
- IT vendor business models were based on proprietary, non-interoperable technical standards. Why? Doctors and hospitals had not been demanding interoperability and modularity; fee-for-service reimbursement rewards higher volumes of services and procedures — not improved quality, outcomes and value.
- Vendor EMR offerings had high prices, high switching costs and created customer lock-in.
- Adoption levels of EMRs for both hospitals and doctors were very low.
2) ONC Gets It Right In Three Major Interpretations and Definitions of HITECH
After the passage of HITECH in February 2009, two schools of thought emerged as to how funds should be spent.
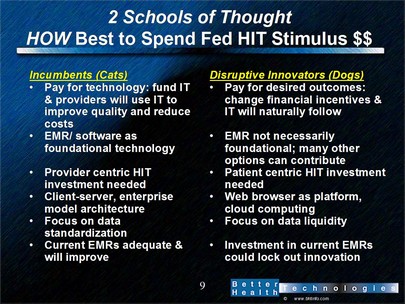
(click on the graphic to view an enlarged version)
One year later, we’re pleased with progress made by ONC in promoting a market that is receptive to innovation.
There were three key interpretations/definitions of HITECH that ONC “got right”. We’ll briefly list and describe each of these; as one way of clarifying the constructive recommendations made by ONC, we’ll start by pointing out what a “wrong” definition/interpretation would have been.
a) Meaningful Use (MU) Emphasizes “Meaningful”, Not “Use”.
The “wrong” interpretation in defining meaningful use would have been to emphasize “use”, rather than “meaningful”. ONC could have defined meaningful use as:
“To achieve MU you must simply buy EMR technology, install it on your server, and train each staff member for 40 hours.”
How did ONC get it right? The definition of meaningful use emphasizes “meaningful” rather than simply use.
- Hospitals and physicians must achieve specific, tangible MU objectives.
- In Phase I, hospitals must achieve 23 MU objectives and physicians must achieve 25.
- Quality metrics have been developed to measure achievement of specific objectives.
Achievement of meaningful use is spread over three phases between 2011 and 2015; the bar for achieving meaningful use will get progressively higher.
2) Vendors Get a Level Playing Field With Certification
The “wrong” recommendation would have been for ONC to default to CCHIT as the incumbent EMR certifying organization and to accept CCHIT’s existing certification process. CCHIT’s process focused almost exclusively on EMR functionality, i.e., does the EMR have specific features.
ONC got it right:
- Certification will be tightly linked to ability to achieve MU.
- Certification will focus on minimum requirements for security, privacy, interoperability, and data exchange.
- The Certification process will be defined by HHS (not by the certifying organization itself). Improve objectivity and transparency of the certification process. Certification to include a range of software sources: Open source, self-developed, etc.
- HHS will designate multiple certification organizations
ONC’s approach improves the objectivity and transparency of the certification process This avoids an appearance of impropriety that a certification organization is too closely aligned with vendors.
c) Lightweight, Open Standards Promote EHR Interoperability and Modularity
The “wrong” recommendation would have been to focus on data standardization instead of data liquidity.
The Standards debate again falls into two schools of thought.
- Standards Drive Adoption: First, focus on creating complex, precise technical standards; these technical standards will drive adoption by users.
- Adoption Drives Standards: First focus on creating data liquidity and moving around existing data; technical standards will evolve.
While intellectually appealing, #1 is just not how things work in the real world of technology adoption. For more details, see the writings by Carol Diamond, Clay Shirky, Peter Neupert/David C. Kibbe, the Markle Foundation, Adam Bosworth, and Steve Waldren/Vince Kuraitis, and others
ONC got it right. The Interim Final Rule for Standard created in December 2009:
- Promotes creation and certification of EHR modules
- Separates patient data from applications
- Emphasizes creation of a lightweight “Health Internet” in building out the Nationwide Health Information Network
- Focuses on data liquidity vs. HITSP-like technical standardization
- Allows both the HL7 CCD and ASTM CCR for summary records
Most recently, Wes Rischel and David McCallie have extended this point of view with their insightful perspectives on “simple interoperability”. Simple interoperability is defining the underlying thinking in the ongoing development of the NHIN-Direct
In the next post in this series, we’ll point out how ONC’s “getting it right” is already transforming the buy (vendor) side of the HIT market.
This work is licensed under a Creative Commons Attribution-Share Alike 3.0 Unported License. Feel free to republish this post with attribution.
Is #HITECH Working? #3: ONC got it right on the 3 major policy interpretations: MU, Cert, Standards http://bit.ly/aUohBd #HealthIT #EHR
Is HITECH Working? #3: ONC got it right on the 3 major policy interpretations.. http://bit.ly/djdW96 (via @VinceKuraitis)
RT @ahier: Is HITECH Working? #3: ONC got it right on the 3 major policy interpretations.. http://bit.ly/djdW96 (via @VinceKuraitis)
RT @VinceKuraitis: Is #HITECH Working? #3: ONC got it right on the 3 major policy interpretations: MU, Cert, Standards http://bit.ly/aUohBd #HealthIT #EHR
#ONC got it right on #MeaningfulUse, #EHR certification, standards … http://bit.ly/aUohBd (HT @VinceKuraitis)
RT @PracticeFusion: #ONC got it right on #MeaningfulUse, #EHR certification, standards … http://bit.ly/aUohBd (HT @VinceKuraitis)
Is HITECH Working? #3: ONC got it right on the 3 major policy interpretations: Meaningful Use, Certification, Standards http://ow.ly/1Axx1