Subscribe if you want to be notified of new blog posts. You will receive an email confirming your subscription.
Finally! CMS Provides a Flood of Details About the Medicare Medical Home Demo
 I’ve been critical in the past when CMS has been silent in explaining their thinking, so I’ll start this post by congratulating CMS on sharing a flood of details about the upcoming Medicare Medical Home Demonstration project.
I’ve been critical in the past when CMS has been silent in explaining their thinking, so I’ll start this post by congratulating CMS on sharing a flood of details about the upcoming Medicare Medical Home Demonstration project.
An email from CMS arrived in my inbox this morning at 2 am. That email notified me that they have updated the MMHD homepage . A quick click lead me to 8 new documents containing 155 pages of newly available details on the MMHD.
If you have time to read just ONE document, take a look a this PowerPoint summary of the MMHD — it’s so fresh that it’s dated October 28, 2008.
Based on a quick perusal, here are some highlights about how the MMHD will be structured. To separate fact from opinion, I’ve put brackets [ ] around my commentary:
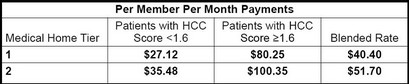
Tiers: There will be two tiers of medical homes (as opposed to the three tiers contemplated in the [good old boy] AMA RUC methodology). [Tier 2 appears to be geared toward getting physicians to adopt EHRs/HIT and to integrate higher levels of systems and processes to improve patient care and care management. This ties the MMHD to broader federal policy objectives.]
Physician Eligibility: “General internist, family practice, geriatrics, most other specialties.” Sorry ER doctors, you’re not eligible. [What were you guys smoking — ER as medical home??].
Patient Eligibility : at least one chronic condition (86% of Medicare beneficiaries). [This is much broader than past care management demos and broader than suggested in the enabling legislation. Overall I think it’s very positive as 1) physician practices would not be motivated to participate if only a very small percentage of their patients were eligible, and 2) the MMHD takes on a much stronger focus on wellness/prevention/early detection.]
Timeline:
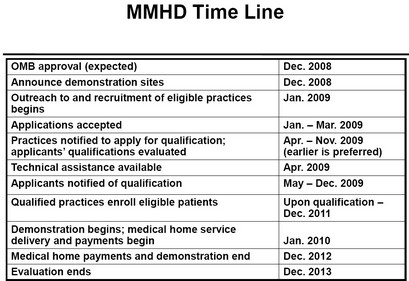
Location and Sample Size
- 8 sites, to be announced in December
- 400 practices
- 2,000 physicians
- 400,000 patients
Application Process:
Practices submit application form (Jan. – Mar. 2009) (under 1 hour to complete application)
Practices submit self-survey tool and documentation of medical home capabilities (Apr. – Nov. 2009) (60–80 hours). [On the plus side, this looks like a thorough process; on the minus side, how many small practices have capabilities/interest to do this?]
Patient enrollment: physicians must enroll eligible patients; both physician and patient must sign medical home agreement.
Care Management Fee: The care management fee will be risk adjusted based on disease burden and predicted future costs to Medicare. [This is probably the most significant newly revealed aspect of the MMHD! The risk adjusted fee of $100.35 per patient per month will provide physicians significant incentives to participate and develop comprehensive care management capabilities. As a reference point, in the Medicare Medicare Health Support demo project, DM companies and health plans were paid care management fees ranging from $80–150 per patient per month.]
Shared Savings: The first 2% of savings are not shared; 80% of savings above the first 2% (minus fees) are shared with participating practices. [This is a highly speculative upside. Doctors, while this potential windfall might look appealing, you might get better odds in Las Vegas.]
Disclaimer — this demo design is not final.
More later….
This work is licensed under a Creative Commons Attribution-Share Alike 3.0 Unported License. Feel free to republish this post with attribution.
Vince, thanks for the post, but I can’t believe that no one has commented yet. Too stunned perhaps?
Steve
Ok, I will be the second one for Vince’s blog.
Medical home is another booming business for small practices if there is a free or low-cost eco-IT system, at least for basic functionalitites that can accommodate the Medicare’s requirement (PHR, PHI, EMR, etc).
Here is the challenge: Medicare-CCHIT’s requirement…… There is no CCHIT’s EMR that can be low-cost or free to meet Medical Home’s requirements.
Ok, let’s take Vista from the VA as an example. $50.00 for the software (I can show you how). Well, even the expert in IT cannot make it run sufficiently . Let’s try to hire a third party vendor. The cost is still tremendous. Ok, got to run for an ER’s pt. I will come back for more. LCN.