Subscribe if you want to be notified of new blog posts. You will receive an email confirming your subscription.
Platform Terminology Explains Why Today’s Patient Portals CAN NOT Work

- Platform Terminology Explains Why Today’s Patient Portals CAN NOT Work
- Today’s Patient Portals CAN NOT Work: An Inability to Capture Network Value
- Today’s Patient Portals CAN NOT Work: Friction ACROSS Portals
- The Missing Ingredient in Today’s Patient Portals: Network Effects
“…the patient portal, as currently architected, is a complete dead-end.”
—John Moore, Founder and Managing Partner, Chilmark Research
Patient portals have tremendous potential — but that potential has not been realized and CAN NOT be realized as portals are currently configured.
An understanding of platform business models and strategy explains why today’s patient portals are inherently suboptimal.
This essay is the first in an occasional series that will look at patient portals through the lenses of platform business models and strategy. Today’s post will introduce and explain platform terminology of multihoming and single homing. Future posts will look more deeply into “why” current patient portals can’t work and will propose options for portals that could work for patients.

Briefly Characterizing Today’s Patient Portals
The Office of the National Coordinator for Health Information Technology (ONC) defines a patient portal as “a secure online website that gives patients convenient, 24-hour access to personal health information from anywhere with an Internet connection.”
Most of today’s patient portals were adopted on the mid 2010’s. They were adopted to comply with ONC’s Meaningful Use regulations for electronic health records. ONC’s mandate for portal adoption by care providers was well intentioned, but misguided. An MGMA survey documented that by 2017 over 90% of care providers had implemented patient portals.
Patient portal adoption and usage has been tepid. ONC’s report published in September 2021 — Individuals’ Access and Use of Patient Portals and Smartphone Health Apps, 2020 — provides some of the latest data.
The ONC survey found that 59% of patients reported having been offered a portal in 2020 and that 38% had actually used one.
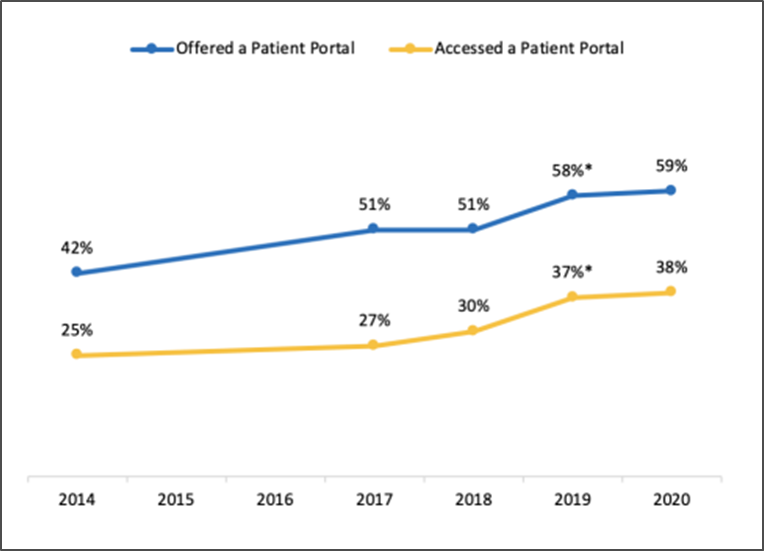
Only 18% accessed the portal 6 or more times.
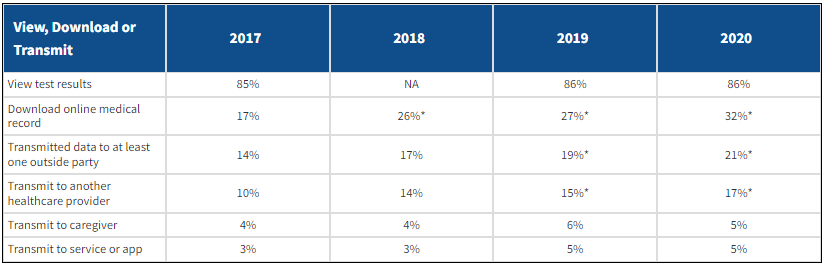
When patients were asked how they used their portal, most of the reported use was transactional — as opposed to being relational and/or used part of a longitudinal clinical care process. As reported by 86% of respondents in 2020, the single greatest use of a portal was simply to review test results.
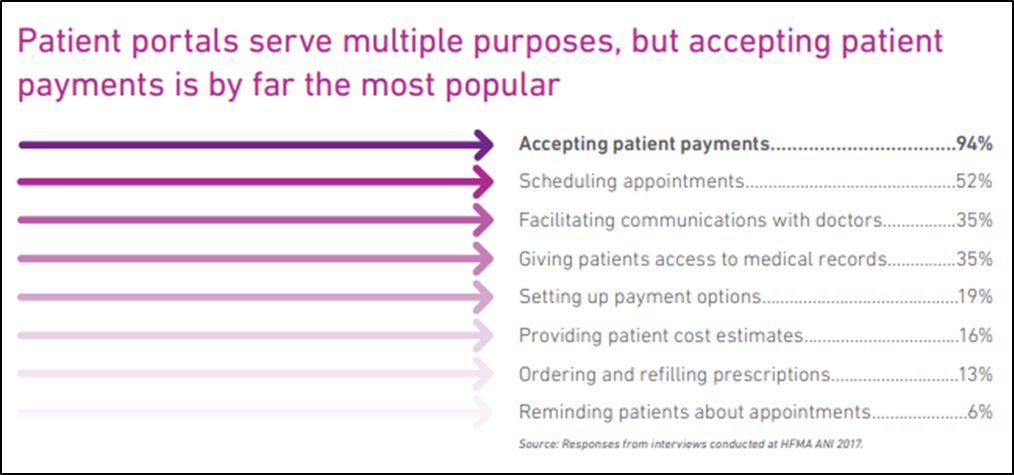
A 2017 Experian survey examined the benefits of patient portals from the hospital point-of-view (vs. the patient POV). The single greatest benefit from the hospital POV was “accepting patient payments”, cited by 94% of respondents. Only 35% of hospital execs saw value in involving patients in their clinical care (e.g., “facilitating communication with doctors” or “giving patients access to medical records”).
By definition, today’s portals are NOT patient-centric — they are tethered to individual provider organizations.
That’s worth repeating:
By definition, today’s portals are NOT patient-centric — they are tethered to individual provider organizations.

Platform Concepts: Multihoming vs. Single Homing
Why can’t today’s patient portals achieve their potential? The key is in recognizing the difference between user preference for “multihoming” vs. “single homing“. Think of it as “How many ‘homes’ are users willing to have for a specific category of platform?
Many platform technologies are amenable to multihoming, i.e., users are comfortable using multiple versions. The utility they gain from a platform isn’t diminished by simultaneously having other similar platforms. Examples where users are comfortable using two or more platforms:
- Subscription video services (e.g., Netflix and Hulu)
- Credit cards (e.g., VISA and MasterCard)
- Securities brokerages (Schwab and Fidelity)
- Newspapers (New York Times and Wall Street Journal)
- e-Commerce (Amazon and Walmart)
BUT…for many platform technologies, users strongly prefer single homing, i.e., ONE home. The greatest utility is derived when users adopt one platform, usually to the exclusion of other platforms. Examples where most users tend toward selecting a single platform:
- Internet service providers
- Cable TV vendors
- Computer operating systems
- Video game consoles
- Smartphones
The terms single homing and multi homing describe strong tendencies or preferences, not hard and fast rules. You could have more than one ISP, computer OS, smartphone — but most people don’t.
Patient portals optimally are single homing platforms – user experience will be suboptimal if they have multiple patient portal homes.
Here’s another way to think about patient portals. Why does Facebook work? For most people, the answer would be something like “Almost all my friends are on the same network”. In other words, Facebook enables a preferred single-homing experience for users.
Your mom wants ONE portal, not seven.
This work is licensed under a Creative Commons Attribution-Share Alike 3.0 Unported License. Feel free to republish this post with attribution.